

Fix the System, Not the People: Why Clinical AI Fails Before It Even Starts
AI won't fix a broken workflow. It will only make the cracks more visible.
Before adding another AI tool, ask a different question:
Is the system ready for it?
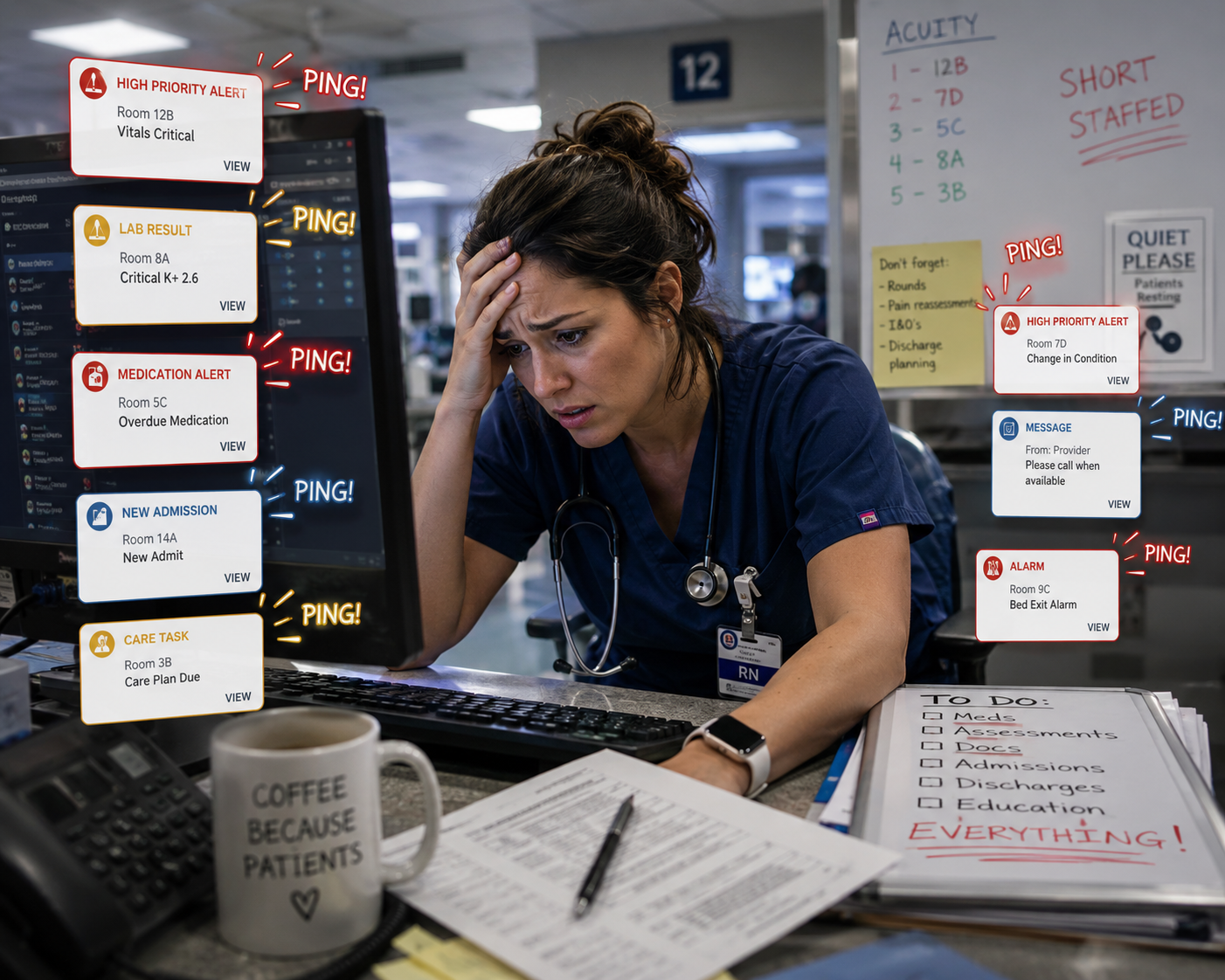
If clinicians are already overwhelmed by alerts, duplicate documentation, disconnected systems, and constant interruptions, introducing AI without redesigning the workflow may increase complexity instead of reducing it.
Fix the system first. Then let AI accelerate what already works.
AI-generated illustration for WB Transformation Consulting.
There's a pattern playing out in healthcare organizations right now, and it's predictable enough to set a clock by.
Throughput stalls. Backlogs grow. Quality metrics start to slip in ways nobody can quite pin down. Leadership responds — reasonably, from where they sit — by looking for a tool. An AI platform gets piloted to triage cases faster, flag documentation gaps, or route patients more efficiently. Six months later, the dashboards haven't moved the way anyone promised. The explanation that circulates is almost always the same: adoption problem. Staff aren't using it right. More training is ordered. A "change champion" gets appointed.
Nobody goes back and asks the only question that actually mattered: was the workflow underneath this tool coherent in the first place?
It usually wasn't. And that's the diagnosis that gets skipped, over and over, because it's easier to retrain people than to admit the system was never built to support what's being asked of it.
The Misdiagnosis Is the Real Problem
When operations and quality functions run on separate logic; different handoff points, different definitions of "done," different owners for the same case at different stages. The gap between them doesn't show up as a system failure. It shows up as a person failure. A case falls through a handoff. A quality flag gets raised two steps too late to matter. A throughput number gets hit by moving a bottleneck somewhere it's less visible, not by resolving it.
Leadership sees the symptom — a person or team missing a beat — and treats it as a performance issue. But the person didn't create the misalignment. The system did. They were operating inside a process where the throughput team and the quality team were never actually looking at the same data, at the same time, with the same definitions.
Layering AI onto that structure doesn't fix the misalignment — it accelerates it. An algorithm that triages faster, on top of a handoff that was already broken, produces confidently wrong outputs faster. The tool gets blamed. The staff get blamed twice — once for the original gap, and again for "failing to adopt" a tool that was never going to work on top of a fractured process.
What Integration Actually Requires
"Integrate throughput and quality workflows" sounds like a slogan until you get specific about what it means operationally. At WB Transformation, this is where the work actually starts, and it's also where we differ from how most of the market approaches this problem.
Most engagements start with a request: "we need an AI tool for X." The vendor response is to build or configure a service and see what returns show up. That's building first and hunting for value afterward — and it's exactly backwards.
We start with three things, in this order, before any tool conversation happens:
Value stream mapping. Before touching a workflow, we map the full value stream — not just the throughput lane or the quality lane in isolation, but where they're supposed to intersect and where they actually don't. This is what surfaces the real bottleneck: it's rarely where leadership thinks it is, and it's almost never a people problem once you can see the whole stream at once.
Process mapping at the handoff level. Once the value stream is visible, we map the specific processes at each handoff point — who owns a case, what "complete" means to them versus what it means to the next function downstream, and where those definitions silently diverge. This is usually where throughput and quality turn out to be optimizing against each other without anyone deciding that on purpose.
Data validation against the actual workflow. This is the step almost everyone skips. Organizations validate data against reports. They rarely validate it against what the workflow is actually doing on the ground. When the two don't match which they frequently don't; Every downstream tool, AI or otherwise, inherits that gap and amplifies it.
This is what "thinking holistically" means in practice. It's not a values statement — it's a sequence. Value stream first, process second, data validation third. Only then does a tool conversation make sense, because only then do you know what the tool actually needs to plug into.
A Simple Example
Picture a nurse partway through a shift. She's got three separate systems flagging her: one for medication timing, one for vitals thresholds, one for care-plan tasks. Each tool does its one job well. None of them talk to each other, and none of them show her the patient as a whole person — just their own slice of the alert queue.
Somewhere in that noise, a note gets logged: a diabetic patient's meal pass was missed. The aide believes the nurse saw it — it's in the system, after all, technically "flagged." But it's flag number forty-something that hour, buried under a stack of lower-priority pings from two other tools competing for the same fifteen seconds of attention. The nurse doesn't recognize it as the one that mattered. The patient doesn't eat until much later than planned. Blood sugar spikes.
Nobody failed to do their job. The aide logged the note. The nurse was working through her queue in good faith. The tools all functioned exactly as designed. What failed was the space between the tools — three systems solving three narrow problems with no shared view of the patient, and no one accountable for the handoff between them.
Add an AI tool on top of this — say, one more layer meant to "prioritize" alerts — and it inherits the same blind spot. It can only rank what it's fed. If meal-pass status, vitals, and care-plan tasks are still living in three disconnected systems, the AI is just adding a fourth voice to an already unmanageable chorus, guessing at priority without the full picture either.
This is the gap value stream mapping is built to find: not "which tool is best," but where a patient's real status gets fragmented across systems that were never designed to reconcile with each other. Process mapping is what shows you the alert actually reached someone — followed by data validation confirming what "reached" meant in practice versus what the workflow assumed it meant. Only once that's visible does it make sense to talk about which tool, if any, actually helps.
No amount of retraining the nurse to "check her alerts more carefully" fixes this. The alerts were never the problem. The absence of one integrated picture of the patient was.
The Sequence Matters More Than the Tool
None of this is an argument against AI in clinical operations. It's an argument about sequence. The organizations that get real value from these tools are the ones that treat workflow integration as the prerequisite, not the cleanup step. Value stream mapping, process mapping, and data validation aren't preamble to the "real" work of tool selection — they are the work that determines whether any tool has a chance of succeeding.
Fix the system first. The people were never the problem.
WB Transformation Consulting works with healthcare organizations on the workforce and organizational effectiveness foundation that has to be in place before technology investments — including AI — can deliver on their promise.